Related

New York Magazine
Press
/ Dec 21,2018
Reducing the Ill Effects of Vaping

NPR
Press
/ Nov 11,2016
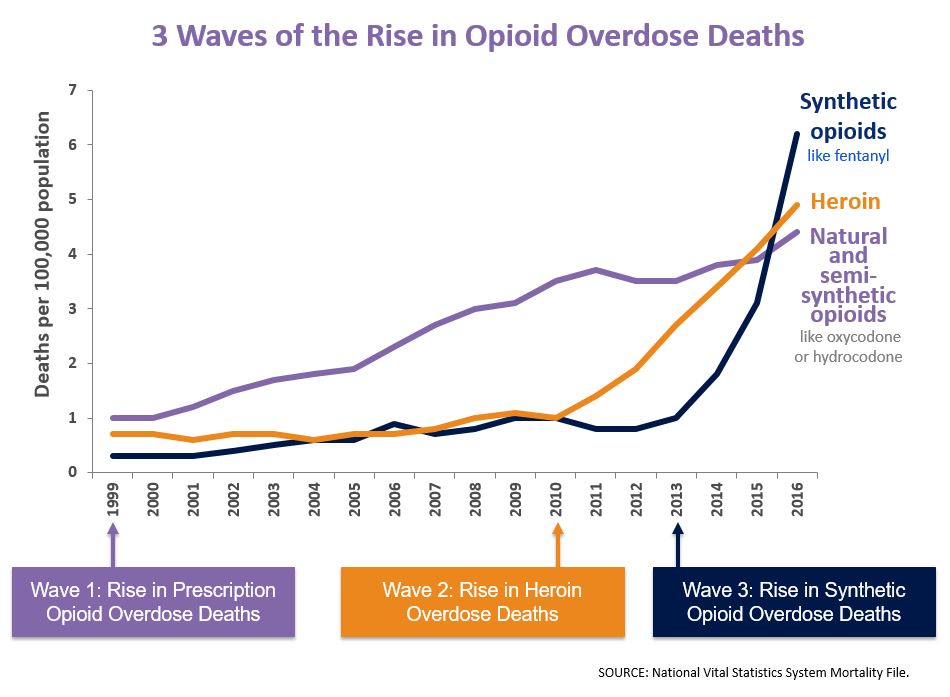
The synthetic opioids - usually referred to both in the press and by law enforcement as "fentanyl" - have now outstripped not only the prescription opioids such as oxycodone but also heroin in terms of overdose deaths, and (as you can see below) the trend line is almost vertical.
Keith Humphreys warns of "fentanyl’s potential to permanently alter illegal drug markets."
Kevin Drum asks about the causes of the change: "Fentanyl has been around for a long time, and only recently has its use become widespread. Why?"
Why, I thought you'd never ask. Settle back; this is a complicated story, and it's going to take a while to tell. But Keith is right: this is a BFD. So it's worth understanding.
First, a little bit of chemistry and pharmacology. "Fentanyl," in its precise use, is the name of a single molecule. It's a purely synthetic opioid: that is, it binds to the same μ opioid receptors as do oxycodone or heroin and has most of the same effects, but it's not made from the opium produced by the poppy plant; its raw materials are chemicals, not crops. It's about thirty times as "potent" as morphine: that is it takes about thirty times as much morphine as it does fentanyl to get the same pain relief. (Here's a handy chart.) Morphine is the standard reference molecule here; note that both diamorphine (heroin) and oxycodone are about 1.5x as potent as morphine itself. Potency also varies with route of administration; injection is about 3x as effective as swallowing a pill.
For a person who hasn't developed a tolerance (and who enjoys the emotional effects of opioids: most people don't) 5mg. of oxycodone (by mouth) is enough to get high on; that's also the dose that will handle moderate pain, and the amount in a Percocet. That same person would likely get the same effect with about 1-1.5 mg. of injected heroin. But it would only take about 1/20th of a milligram - that's 50 micrograms - of injected fentanyl.
In medical practice, injected fentanyl is most common as part of surgical anaesthesia; as a pain reliever - generally for people with severe, chronic pain - it's more usually administered as a transdermal patch from which the molecule gradually leaches into the bloodstream, or as a lozenge.
But the "parent" fentanyl compound turns out to be one member of a very large chemical family, known generically as "fentanyls," each with its own name and a varying set of pharmacological properties. Some of them are astoundingly potent: carfentanil, for example, has something like 100 times the potency of fentanyl itself, which makes the effective dose for a human a fraction of a microgram. (And yes, it's literally used - in dart guns - as an elephant tranquilizer.) Legally, those other molecules are "fentanyl analogues."
The opioids as a class have what is known as a "narrow therapeutic window," where the "window" is the range between the median effective dose (ED50) - the dose that's has the desired effect in half the population - and the median lethal dose (LD50). The larger the LD50/ED50 ratio (the wider the "window") the safer the drug will be in terms of overdose risk.
For the opioids, the ratio (also called the "therapeutic index") is typically about six, which sounds like a reasonable margin of safety until you remember that individuals differ, that individual vulnerabilities differ from occasion to occasion (especially with the presence of other drugs, notably alcohol), and that people make mistakes, especially when drugs are made and distributed illicitly rather than in pharmaceutical factories and taken by people who are not always operating at their cognitive peak. Given all that, a factor of six is an uncomfortably narrow window.
The narrow therapeutic window explains why overdose death is so much more common with the opiods than with the stimulants or the benzos or alcohol. And the smaller the intended dose, the harder it is to measure out precisely. So high potency, which can be an advantage clinically (allowing less painful injections and the use of things like transdermal patches) can be a nightmare on the street. To make things even worse, neither users nor dealers have reliable ways of knowing just what's in the white powder they're consuming or selling: someone who injects what he thinks is the right dose of heroin, but has in fact purchased fentanyl, is likely to stop breathing. Even someone who intends to take fentanyl could die if he's actually been given, say, 3-methylfentanil or some other high-potency analogue.
Which - finally - brings us back to Kevin's question: "Why is this stuff just getting popular now?" Fentanyl was patented as a pharmaceutical nearly 60 years ago. It was in limited use as a street drug - some diverted from medical use, some illicitly synthesized (back then, mostly domestically) by the early 1980s. From a trafficker's viewpoint, high potency meant high value-to-bulk, making it much easier to ship illegally without getting caught. But from a user's viewpoint, it was Russian Roulette. A street dealer buying fentanyl from a higher-level supplier and "stepping on it" - diluting it with mostly inert chemicals - would have needed remarkable skill to ensure that every dose had just 50 micrograms of the active agent and that none had the 300 micrograms - roughly the weight of a grain of table salt - that could be deadly. So fentanyl never really caught on.
At the same time, the price of heroin started to fall, and kept falling. In 1979, a milligram of pure heroin delivered to an illegal consumer in the U.S. sold for about $2.40; that's something like $9 in today's money. Today, that same milligram sells for something less than a quarter. The causes of that decline - and similar declines seen over the same time period in the prices of cocaine and cannabis (adjusted for its rising potency) - aren't entirely clear. It certainly hasn't been for want of vigorous enforcement; we have about thirty times as many drug dealers behind bars today as we had in 1980 (450,000 v. about 15,000). My guess is that it's mostly learning-by-doing: over time, drug dealers develop smoother and smoother procedures for doing business and avoiding enforcement, helped along by the falling prices of transportation and information and the rising volume of international and long-distance commerce. (Falling homicide rates also reduced one major risk of drug-selling.)
Then we got hit with the wave of prescription-opioid (mostly hydrocodone and oxycodone) diversion and dependency that started around 1992 and was accelerated by the introduction of Oxycontin in 1996, and its relentless marketing by Purdue Pharma. The widespread availability of diverted prescription opioids - available in pharmaceutical bottles, in every neighborhood, often from friends or at least from people who didn't look as scary as old-fashioned heroin dealers, and cheap enough to be taken orally rather than by the more efficient, but ickier, injection route - created a widespread national demand for opioids. As those oxycodone users built up habits they could no longer afford, or lost access to their favorite script-happy M.D. or "pill mill" pharmacy, the falling price of heroin enticed many of them to "trade down." Milligram-for-milligram, heroin cost about a quarter as much as oxycodone (25 cents vs. a dollar). The 2011 reformulation of Oxycontin - a high-dose, time-release form of oxycodone, whose time-release feature turned out to be trivially easy to circumvent and which could be dissolved and then injected - into a less-easily-abusable form accelerated the transition from pills to strictly illegal street drugs.
At the same time, people in the U.S. were learning how to buy chemicals unavailable here - banned drugs, cheap unbranded pharmaceuticals, Human Growth Hormone, you name it - by mail-order from illicit or quasi-licit outfits in China, ordering over the Internet (and, when law enforcement made that dangerous, over the "Dark Web") often paying in cryptocurrencies. Instead of using complicated smuggling schemes, sellers simply put these products in the mail; for about $20, you can get a package of up to four pounds mailed from China to New York.
It didn't take long for some of those Chinese outfits to start making fentanyl; unlike heroin dealers, they didn't need a source of opium. The chemistry involved isn't especially challenging (not, for example, like making LSD). Fifty grams of fentanyl - just over an ounce and a half - has the punch of a kilogram of heroin, and it's way, way cheaper.
Somewhere in here someone figured out a technique for diluting the stuff with enough accuracy to reduce the consumer's risk of a fatal overdose: far from perfectly, but enough to create a thriving market. (I don't know what that technique is, though I can think of at least one way to do the trick.) And for a retail heroin dealer, the financial savings from buying fentanyl (or an analogue) rather than heroin, and the convenience of having the material delivered directly by parcel post rather than having to worry about maintaining an illegal "connection," constituted an enormous temptation. More sophisticated regular consumers sometimes buy direct for their own consumption, saving money by cutting out all of the middlemen.
For law enforcement, the parcel-post approach makes a hard problem nearly impossible. The volume of legitimate parcel post from China to the U.S. means that there's no way to scan every package, or even a high enough fraction to make the traffic uneconomic. As more and more potent molecules appear, I'd expect another shift, from parcel post to regular international mail, moving the drugs in quantities of a gram or less, either just putting a tiny Baggie with the powder inside in the envelope, or perhaps dissolving the drug, soaking a sheet of ordinary paper in the solution, typing a letter on the paper, mailing it, and then extracting the drug at the other end of the process.
So that's why the fentanyls are a big factor now when they weren't before. And I don't see a snowball's chance in Hell of stopping the flow. It's possible that, with adequate urging from the U.S., the Chinese authorities might succeed in cracking down on illicit manufacture and sale. But there's nothing magical about China. India also has skilled chemists and a huge flow of mail to the U.S. So, for that matter, does Canada. And so does the U.S.; if international sources dry up, the stuff will, once again, be made here.
On top of that, the "technology" of illicit retail drug distribution has been transformed by the introduction of mobile phones.
Thirty years ago, illicit retail drug transactions were characteristically carried out either in public locations (parks or street corners) or in dedicated drug-dealing locations (e.g., crack houses). Those locations tended to cluster heavily in low-income, high-crime urban neighborhoods where police had other priorities and neighbors were reluctant to call the police. Having to travel to such a location – risking arrest or robbery – constituted a significant barrier to illicit acquisition. Moreover, for open-air transactions, a buyer had to search for a willing seller–usually, a seller with whom he had an established connection – and that search took time (45 minutes was not uncommon) and sometimes failed entirely. Search time and risk constituted a second kind of “price” of illicit drugs, perhaps as significant (especially to new consumers) as the money price.
From the retailer’s point of view, that style of dealing meant exposure to both enforcement risk and the risk of robbery. It also greatly decreased the number of transactions a dealer could consummate in an hour, since most of his time was spent waiting for customers to arrive. Much of the retail price of illicit drugs represented compensation to the retail dealer for those risks and costs.
But with mobile phones, texting, and social media, transactions can now be arranged electronically and completed by home delivery, reducing the buyer’s risk and travel time to near zero and even his waiting time to minimal levels. In the recent Global Survey on Drugs, cocaine users around the world reported that their most recent cocaine order was delivered in less time, on average, than their most recent pizza order.
These efficiencies reduce retailer’s costs and thus the margins they need to earn to stay in business. That in turn reduces the retail price. Bottom line: the stuff is cheap and easy to get, just about anywhere in the country. And, again, a user who doesn't have a dealer can become his own importer.
So I'm tempted to reach a fairly grim conclusion: The "supply side" of current drug policy tries to prevent people from harming themselves by falling into substance use disorder (often harming others in the process) through making abusable drugs more expensive and harder to get by making laws against selling them and enforcing those laws. That becomes a less and less workable policy over time.
And no, I don't believe in "drug prevention" (or in the Tooth Fairy). Making people genuinely resilient in the face of temptation can't be done by chanting "Just Say No," or by inventing ever more creative lies to tell to schoolchildren. Lots of people are going to be addicted, when strongly habit-forming and highly pleasurable drugs are available to them, for the same reason lots of them are going to wind up obese when they're offered all the sweet, fatty, and salty food they can stuff themselves with, plus unlimited sedentary amusements.
Fixing that means making serious cultural changes. Over fifty years of struggle, we've made some serious progress on that with tobacco, but tobacco is still much more widely used than any of the illicit drugs except for cannabis. Changing customs is hard work, and it doesn't happen quickly.
In the meantime, all we can do - maybe - is make it easier for people who want to use heroin and not the fentanyls to tell the difference by allowing them to have test kits, and maybe make the penalties for selling much higher for fentanyls than for heroin to give dealers a disincentive. But I wouldn't bet the farm either that we will do those things or that they would work if we did them.
So I think we're going to wind up just making sure that naloxone is available to reverse as many otherwise-fatal overdoses as possible (it's already reversing more than half) and that methadone and buprenorphine are available to help people with opioid dependency when they're ready to stop risking their lives.
It's likely that the current opioid epidemic will burn itself out, as the younger brothers and sisters, and children, of today's problem opioid users decide to profit from the bad example of their elders. But the fentanyls aren't going to be the last class of purely synthetic and super-potent recreational chemicals; they're just the first.
Cross-posted from Reality Based Community.
Tile photo by Dmitri Popov.
Please fill out the information below to receive our e-newsletter(s).
*Indicates required.